Sports Medicine & amp; Arthroscopy
Indications:
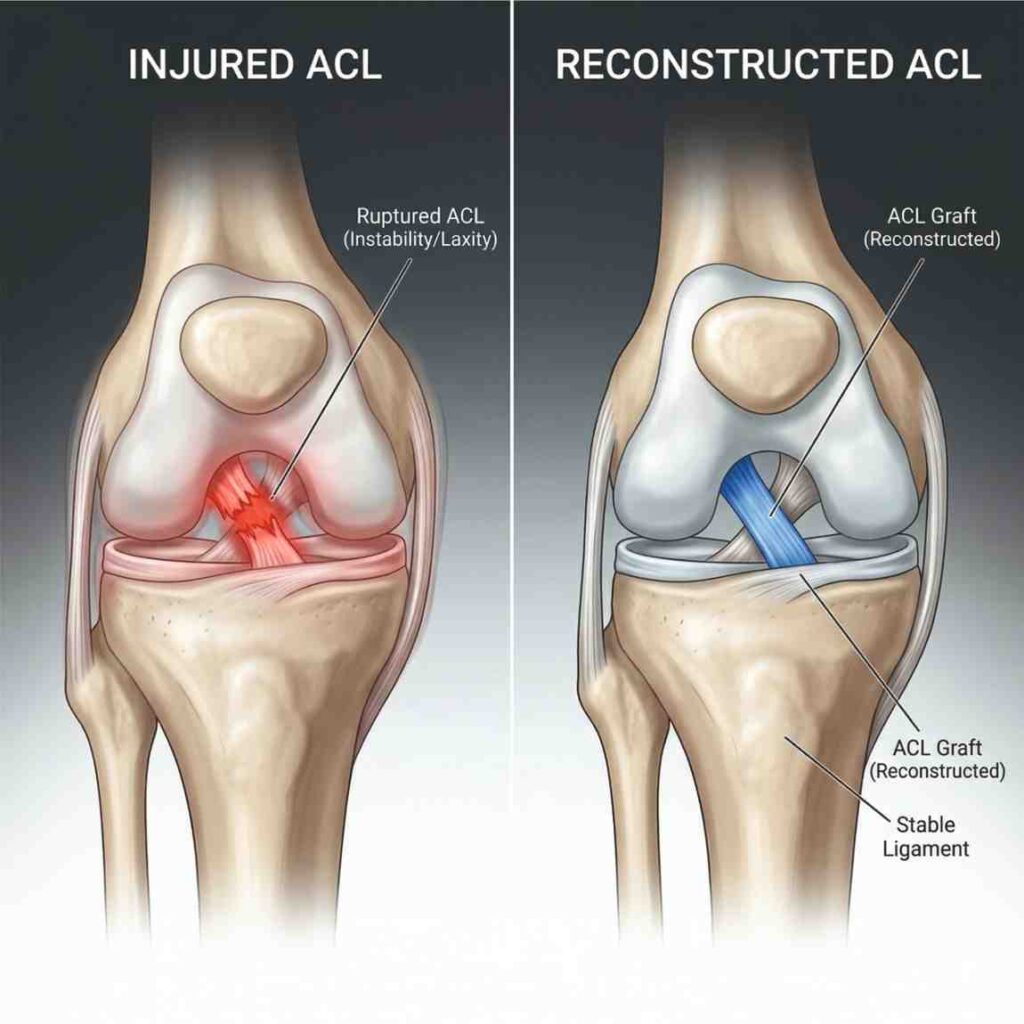
Anterior Cruciate Ligament (ACL) reconstruction is recommended for patients experiencing functional instability of the knee, commonly described as a “giving way” sensation during walking, turning, or pivoting movements. It is particularly important for young, active individuals and athletes who wish to return to sports that involve sudden direction changes such as football, cricket, or basketball.
ACL injury often occurs due to twisting trauma, sports injuries, or accidents. In addition to instability, patients may experience swelling, reduced confidence while walking, and difficulty performing high-demand activities. Surgical reconstruction is generally advised when conservative treatment fails to restore stability or when there is a clear need to return to an active lifestyle.
Technique:
The procedure is performed arthroscopically using minimally invasive techniques under strict sterile conditions. An anatomic ACL reconstruction is carried out to closely replicate the natural ligament structure and function.
A suitable graft is selected, which may include an autograft (patient’s own patellar tendon, hamstring tendon, or quadriceps tendon) or, in selected cases, an allograft. The surgeon carefully prepares the graft and creates precise tunnels in the tibia and femur at the native ACL footprint to ensure proper alignment.
The graft is then passed through these tunnels and secured firmly using fixation devices such as interference screws, cortical buttons, or cross-pins. Proper tensioning and positioning are confirmed to achieve optimal knee stability before completing the procedure.
Objective:
The primary objective of ACL reconstruction is to restore both anterior-posterior and rotational stability of the knee joint. By stabilizing the knee, the procedure helps prevent further damage to important structures such as the menisci and articular cartilage.
It allows patients to regain confidence in knee movement, return to sports activities safely, and maintain long-term joint health with reduced risk of early arthritis.
Arthroscopic Rotator Cuff Repair in Hisar
Indications:
Arthroscopic rotator cuff repair is indicated in patients with full-thickness rotator cuff tears or symptomatic partial tears that do not respond to conservative treatment. Common symptoms include persistent shoulder pain, especially at night, weakness during overhead activities, and difficulty lifting or rotating the arm.
These tears may result from acute injury, repetitive overhead activity, or age-related degeneration. Surgery is usually recommended when pain interferes with daily life or when there is progressive weakness affecting shoulder function.
Technique:
The procedure is performed using advanced arthroscopic techniques through 3–4 small portal incisions, each approximately 1 cm in size. A high-definition camera (arthroscope) is inserted to visualize the shoulder joint clearly.
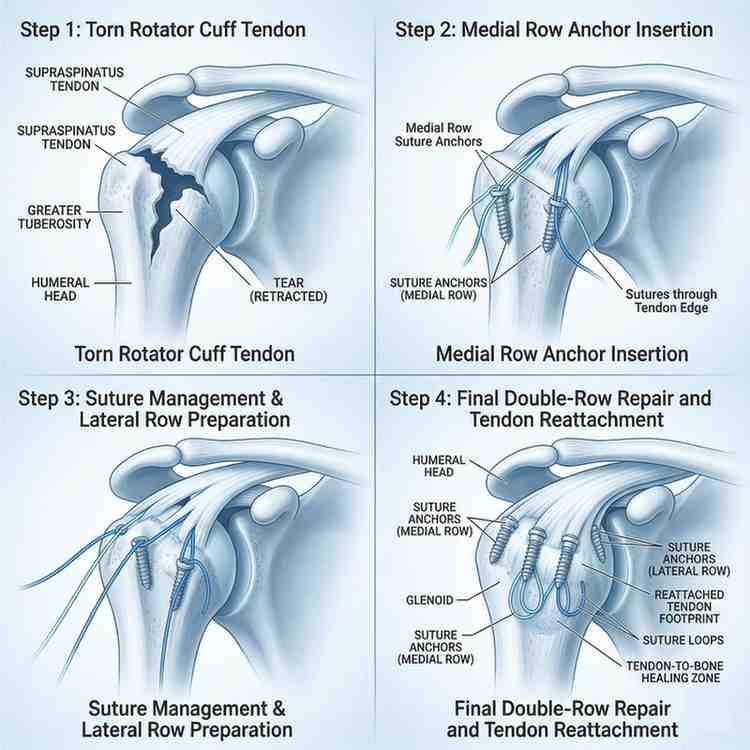
The subacromial space is first cleared by removing inflamed bursal tissue (bursectomy) to improve visibility and reduce irritation. The torn tendon edges are then carefully debrided to create a healthy, bleeding bone surface that promotes healing.
A strong and stable repair is achieved using techniques such as the “double-row” or “suture bridge” method. In this approach, suture anchors are placed into the humeral head, and the tendon is securely reattached to the bone, maximizing the contact area for better healing and long-term strength.
Objective:
The main objective of arthroscopic rotator cuff repair is to restore the normal biomechanics of the shoulder by re-establishing the force couples responsible for smooth and coordinated movement.
This results in significant pain relief, improved shoulder strength, and restoration of overhead function. The procedure enables patients to return to their daily activities with better mobility and long-term joint stability.
1. When is ACL reconstruction surgery necessary?
ACL surgery is usually needed when the knee feels unstable or gives way during daily activities or sports. It is especially recommended for active individuals who want to return to running, jumping, or pivoting movements.
2. How long does it take to recover after ACL surgery?
Initial recovery takes a few weeks, but full rehabilitation usually takes around 6–9 months. Return to sports depends on strength, stability, and physiotherapy progress.
3. Can I walk after ACL reconstruction?
Yes, most patients start walking with support within a few days after surgery. Gradual weight-bearing is increased as healing progresses.
4. Which graft is best for ACL reconstruction?
Common options include hamstring, patellar tendon, or quadriceps tendon grafts. The choice depends on patient age, activity level, and surgeon preference.
5. Is physiotherapy important after ACL surgery?
Yes, physiotherapy is essential for regaining strength, flexibility, and knee stability. It plays a major role in overall recovery.
6. What are the common symptoms of a rotator cuff tear?
Patients often experience shoulder pain, especially at night, weakness while lifting the arm, and difficulty with overhead activities.
7. Is rotator cuff repair done through open surgery?
Most repairs today are done arthroscopically using small incisions, which reduces pain and allows faster recovery compared to open surgery.
8. How long does recovery take after rotator cuff surgery?
Recovery usually takes around 3–6 months. Initial healing requires rest and sling support, followed by structured physiotherapy.
9. Will I regain full shoulder strength after surgery?
In most cases, patients regain good strength and function, especially if rehabilitation is followed properly.
10. When can I return to normal activities?
Light activities can be started early, but heavy lifting and sports may take a few months depending on healing.